Interproximal Papilla in the Esthetic Zone Combining Guided Tissue Regeneration and Soft Tissue Graft. A 7-Year Follow Up Case Report
- 1. Department of Periodontology, Columbia University, USA
Abstract
This case report shows regeneration of the papilla in an advanced interproximal horizontal defect between a maxillary left central and lateral incisor. The therapy consisted in Guided Tissue Regeneration using autogenous bone chips and a resorbable collagen membrane covered with a palatal sliding connective tissue pedicle flap.
A 7 years follow-up shows complete radiographic defect fill, probing depth elimination and full regeneration of the papilla. This case report clinically supports the use of a combined regenerative and mucogingival procedure to regenerate hard and soft tissues in the interproximal area to recreate the papilla in the esthetic area.
Keywords
• Guided Tissue Regeneration
• Papilla
• Autologous Graft
• Resorbable Membrane
CITATION
Amato F (2024) Interproximal Papilla Regeneration in the Esthetic Zone Combining Guided Tissue Regeneration and Soft Tissue Graft. A 7-Year Follow-Up Case Report. JSM Dent Surg 6(1): 1041.
BACKGROUND
In this clinical case, the patient who had been treated for several years with a program of periodic oral hygiene maintenance through scaling and root planing had already lost the papilla in between her maxillary central and lateral incisor. Therefore, the challenge was not only to regenerate the periodontal attachment but also to recreate the papilla.
CLINICAL PRESENTATION
In April of 2021, her dentist because of some tooth extrusion referred a 45 years old female and recession had taken place on crown # 9 and 10 showing the metal border and the interproximal papilla had disappeared. Furthermore, a disto-palatal periodontal pocket was still present on her maxillary left central incisor despite the 4-5 months periodic oral hygiene maintenance visits and the good oral hygiene conditions.
The patient chief complaint was to improve the esthetic of her smile.
Medical history revealed the patient to be in good health conditions and a non-smoker.
Dental history revealed that on tooth # 9,10 a two units PFM bridge was fabricated about 20 years previously due to extensive cavities on the teeth. Patient showed full compliance with the hygiene maintenance program during the past years.
Clinical examination showed good oral condition and a full natural dentition, absence of periodontal disease in the rest of the mouth.
Periodontal examination revealed full mouth in healthy condition with the exception of tooth # 9 and #10, absence of plaque or calculus and a thin and scalloped biotype (Figure 1).

Figure 1: The patient presented with a t 8 mm loss of attachment distal on maxillary left central incisor: 3 mm of recession and 5 mm of probing pocket depth distally and palatally.
The maxillary left central and lateral incisors had extruded for about 2 mm, had moderate gingival inflammation, 2 mm of recession both on the palatal and the buccal side, bleeding on probing, 5 mm of probing depth interproximally and complete absence of the interproximal papilla (Figure 2 and Figure 3).

Figure 2: The maxillary left central and lateral incisors had extruded for about 2 mm, had moderate gingival inflammation
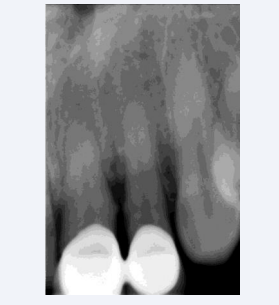
Figure 3: X-ray examination showed advanced horizontal bone loss of the interproximal area between tooth # 9 and #10.
A diagnosis of localized moderate periodontal loss of attachment with an horizontal bone defect interproximally on tooth # 9 and 10 was done and a guided tissue regeneration periodontal therapy combined with a soft tissue augmentation surgery to recreate the papillary tissues was planned.
CASE MANAGEMENT
One month after initial therapy and oral hygiene instruction and motivation A new acrylic resin provisional was fabricated and the periodontal surgery was scheduled.
72 hours before periodontal surgery full mouth scaling was done and patient was prescribed chlorexidine to rinse three times a day for two weeks.
Antibiotic prophylaxis (amoxicilline 1 gr.) was prescribed for the patient to take twice a day for ten days starting 12 hours prior to surgery
After local infiltration with Articaine 1:100.000 an intrasulcular incision was carried out on the maxillary left central, lateral and canine both vestboularly and palatally and two vertical releasing incision were made buccally extending beyond the mucogingival line in order to expose the alveolar bone for autologous bone harvesting.
After raising a full thickness flap a thorough debridement of the defect was performed showing a no-walls defect interproximal between central and lateral incisor. Autologous bone curls were scraped from the alveolar bone apical to the root apexes and carefully molded in the defect to recreate the original bone architecture. The graft was then covered with a resorbable membrane shaped to be adapted to the interproximal area as well as buccally and palatally. A palatal pedicle flap was raised and rotated interproximally and buccally to cover the membrane and recreate the papilla and then sutured on the inner aspect of the vestibular flap.
A full thickness mucoperiosteal flap was raised. After a thorough debridement a 5 mm horizontal osseous defect was visible on the interproximal area between tooth # 9 and 10.
A careful scaling and root planing of the root surfaces was performed using rotary instruments, ultrasonic tips (Piezosurgery Mectron) and manual curettes (Hartzel &Son) (Figure 4).

Figure 4: A careful scaling and root planing of the root surfaces was performed using rotary instruments, ultrasonic tips (Piezosurgery Mectron) and manual curettes (Hartzel &Son)
Autologous bone was harvested from the alveolar bone apical to the root apexes with a bone scraper (Safescraper META advanced medical technology).
The harvested bone curls were immediately grafted in the defect and molded in the attempt to recreate the original bone architecture of the interproximal area.
A resorbable membrane (Osseoguard 15x30 3i BIOMET) was trimmed and shaped to be adapted to the interproximal area and fully cover the graft material both on the buccal and palatal side (Figure 5 and Figure 6).

Figure 5: A resorbable membrane (Osseoguard 15x30 3i BIOMET) was trimmed and shaped to be adapted to the interproximal area.
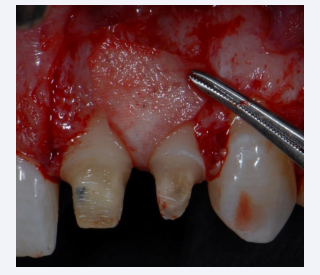
Figure 6: Palatal pedicle flap to rebuild the interproximal papillary soft tissue
Periosteal scoring incisions were performed to allow flap release and to ensure tension-free flap closure (Figure 7).

Figure 7: Periosteal scoring incisions were performed to allow flap release and to ensure tension-free flap closure.
The flap was then closed using a fine suture (Ethicon propylene 6-0), in the anterior area and a thicker suture (Ethicon silk 4-0) in the area posterior to the canines (Figure 8).

Figure 8: The flap was then closed using a fine suture (Ethicon propylene 6-0), in the anterior area and a thicker suture (Ethicon silk 4-0) in the area posterior to the canines.
In the interproximal area vertical mattress sutures were applied while in the posterior area simple interrupted sutures were used (Figure 9).

Figure 9: In the interproximal area vertical mattress sutures were applied while in the posterior area simple interrupted sutures were used.
The patient was seen once a week for the following three weeks for suture removal and hygiene maintenance in the wound area and then once a month for recall visits.
Clinical Outcome
Seven years after surgery radiographic examination revealed good defect fill. Clinical examination showed absence of inflammation and 2 mm probing depth and a newly regenerated papilla (Figure 10).

Figure 10: Frontal view showing clinical conditions before and at 7-Year follow up.
Periapical x-rays showing interproximal bone peak before treatment and at 7-Year follow-up. Notice the complete vertical regeneration (Figure 11).
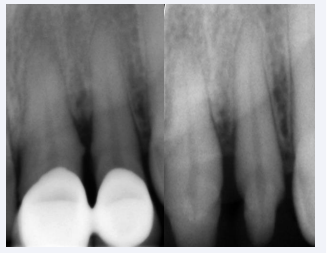
Figure 11: X-rays showing interproximal bone peak before treatment and at 7-Year follow-up.
DISCUSSION
Periodontal disease is often treated with scaling and root planing alone or in combination with open flap debridement [1]. Elimination of inflammation and repair of soft tissue upon healing together with oral hygiene maintenance program allows to prevent the periodontal disease progression [2]. Although with this pocket reduction/elimination approach predictable and stable results have been documented, in the esthetic area the consequences are often not well accepted by the patient.
In fact the” black triangle disease”, the increase of recession - which is usually accompanied by tooth sensitivity, dyschromia, and tooth elongation - are often side effects of periodontal treatment [3,4].
Guided tissue regeneration is the ideal alternative treatment to recreate the periodontal attachment that has been lost due to periodontal disease [5]. However, a vertical component of the defect with intact bony walls together with the use of a selective tissues barrier and a sufficient healing time with stable membrane coverage are necessary in order to obtain recreation of periodontal tissue. Furthermore the use of a membrane, which is necessary for tissue regeneration, may result in negative effects such as infection, premature membrane exposure, loss of the graft and recession [6,7].
The possibility to achieve tissue regeneration in the esthetic area represents a great challenge for the periodontist. Deep biological knowledge, good skills and adequate surgical tools represent the key to predictable success [7]. Autogenous bone is considered the gold standard material for bone regeneration [8]. In this case the autogenous bone chips were harvested form the area neighbouring the defect with a bone scraper. The advantages of using GTR membranes are that resorbable membranes do not require a second surgical site and reduce patient morbidity, help in soft tissue healing, show tissue friendly reactions to membrane exposure, and are cost-effective [9]. To achieve complete coverage of the membrane is necessary to use a connective graft augmentation, but in the interproximal area the blood supply is limited and may impair the survival of the soft tissue graft. To overcome this problem in this case a rotated split palatal flap was applied to maintain the blood supply of the interproximal grafted tissue [10]. In this case careful management of the soft tissue in the papillary area together with the use of fresh autologous bone chips and the application of a membrane that allows for easy handling, good adaptation and optimal tissue integration appear to have had a relevant role in the clinical success [11].
CONCLUSION
The case report demonstrate the clinical success of using of a resorbable membrane and autologous bone chips in combination with a palatal sliding pedicle flap to regenerate an interproximal defect and recreate the papilla in the esthetic zone. More data and larger number of cases are necessary to further validate the results of this study.






































































































































